Preoperative Bronchoscopy in Esophageal Atresia: Unmasking a Proximal Tracheoesophageal Fistula
Abstract
Background: Preoperative bronchoscopy is not universally performed for primary repair of esophageal atresia (EA) but may aid with localization of tracheo-esophageal fistulas (TEF), detect associated airway abnormalities, and reduce the risk of missed additional fistulas.
Methods: We report a neonate with EA who underwent dynamic flexible bronchoscopic evaluation prior to primary repair. Initial bronchoscopy under spontaneous breathing assessed the larynx, trachea, airway collapsibility and localized the suspected distal TEF. The examination was continued via laryngeal mask airway (LMA), using positive end expiratory pressure (PEEP). In addition, low-flow oxygen jets were applied via the working channel to explore for further TEFs.
Results: A TEF was identified approximately 2 cm above the carina, with severe posterior intrusion type tracheomalacia at the same level. Using an LMA with 10 cm H2O PEEP and 2 L/min bronchoscopic oxygen jet insufflation, a second, more proximal fistula became visible approximately 2 cm above the distal fistula. Additional intraoperative bronchoscopy after repair confirmed successful closure of both fistulas.
Conclusion: Preoperative bronchoscopy may improve anatomical mapping and perioperative planning in EA. Detection of a fistula should not conclude the evaluation; additional fistulas require deliberate exclusion. PEEP and low-flow bronchoscopic oxygen insufflation may help expose occult fistulas.
Video
Introduction
Preoperative bronchoscopy in newborns with esophageal atresia remains non-uniformly practiced across centers. Its potential value lies in defining fistula location and anatomy, identifying tracheomalacia and other tracheolaryngeal abnormalities (1), and reducing the risk of missed additional, usually proximal, fistulas. In a review by Parolini et al. from more than a decade ago (2), preoperative tracheobronchoscopy was described as valuable, but still debated and not routinely incorporated into diagnostic and surgical assessment in many centers. More recent consensus recommendations (3) support routine tracheoscopy before operation to evaluate the fistula(s) and associated tracheolaryngeal pathology.
A key technical challenge is the presence of an occult or collapsed proximal fistula, which may evade detection on initial inspection. Accordingly, systematic preoperative airway endoscopy has been advocated, given the high prevalence (1) of associated laryngotracheal abnormalities that can influence management. In this context, flexible bronchoscopy performed under spontaneous breathing allows concurrent assessment of vocal cord motion and tracheomalacia; however, identification of a proximal fistula – particularly when collapsed – may require adjunctive techniques to transiently distend the airway and unmask the lesion.
This video article highlights a practical bronchoscopic approach, demonstrating how modification of airway conditions – specifically the application of PEEP and low-flow oxygen insufflation – can aid detection of an otherwise occult proximal fistula, with direct implications for diagnostic accuracy and perioperative decision-making.
Case Description
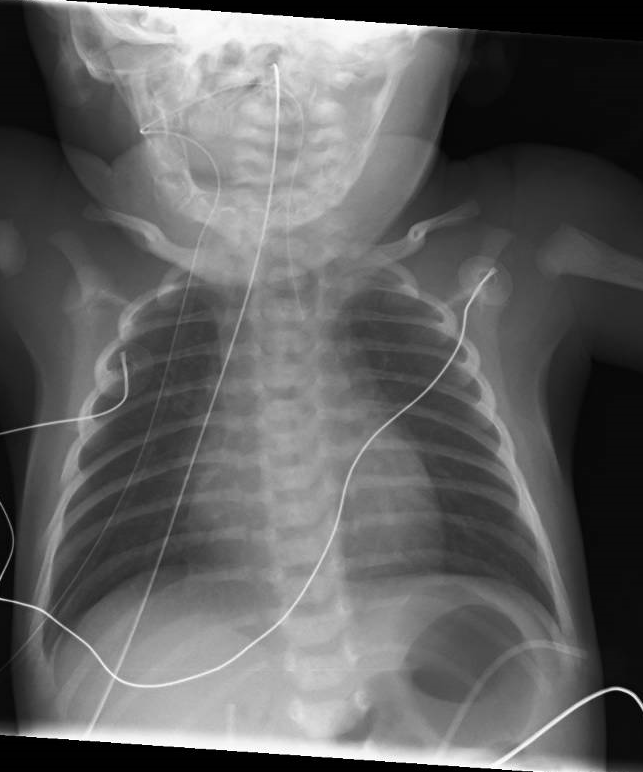
A male neonate was born at 36 weeks' gestation. Postnatally, EA was diagnosed, with the presence of gastric air raising suspicion for a tracheoesophageal fistula (figure 1). At 5 days of age, the patient proceeded to surgery.
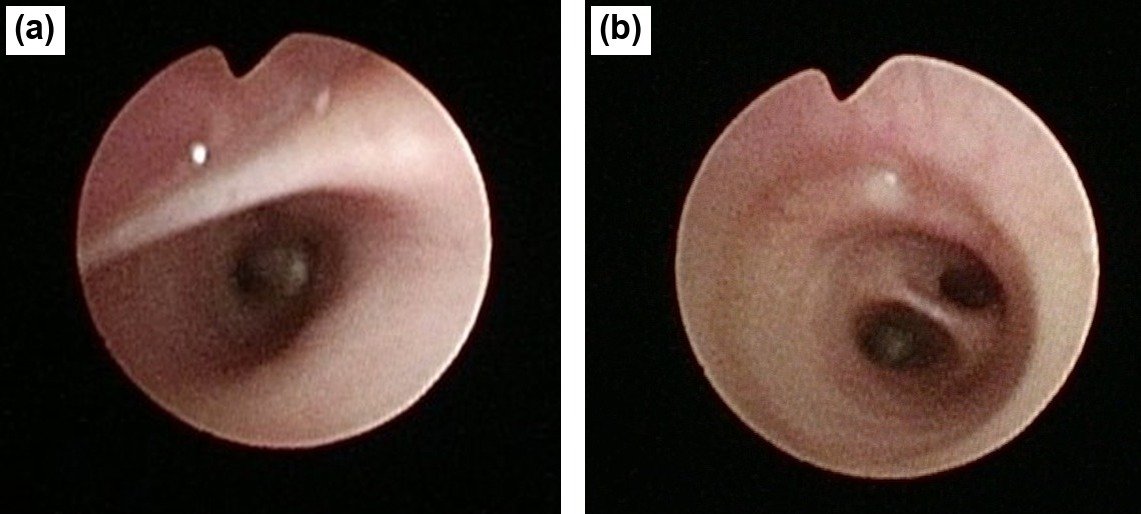
Preoperative bronchoscopy was conducted in two stages, using a 2.8-mm flexible bronchoscope with a 1.2-mm working channel (BF-XP190, Olympus Medical Systems, Tokyo, Japan). Initially, flexible bronchoscopy was performed via nasal passage under spontaneous breathing, allowing assessment of laryngeal anatomy and dynamic tracheal behaviour. Vocal cord mobility and laryngeal structures appeared normal. Direct laryngotracheal palpation was not undertaken; therefore, the presence of a subtle low-grade laryngeal cleft could not be definitively excluded. At mid-tracheal level (T2), there was severe tracheomalacia of posterior intrusion type, with ~90% luminal narrowing (figure 2). The proximal (T1) and distal (T3) tracheal segments were patent without evidence of malacia, and bronchial anatomy was normal. The bronchoscope was rotated to align the posterior membranous wall with the upward-flexed aspect of the scope, to optimize the viewing angle and improve both visualization and control. A fistulous opening was visualized on the posterior tracheal wall approximately 2 cm above the carina; however, its presence, precise location, and size could not be reliably defined due to intermittent tracheal collapse obscuring the view. Notably, even during transient airway expansion during inspiration, the fistula did not consistently open, suggesting a dynamic, pressure-dependent or flap-valve configuration with intermittent occlusion (figure 3a).

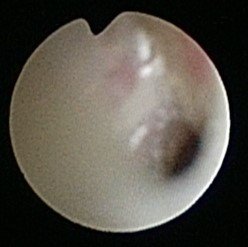
The examination was subsequently continued through an LMA under PEEP of 10 cm H2O. Low-flow oxygen jet insufflation was applied intermittently through the bronchoscope working channel, at 2 L/min as previously described (4). Insufflation was brief, targeted, and discontinued once the fistulas were identified. Continuous cardiorespiratory and pulse oximetry monitoring were maintained, and high-pressure jet ventilation was avoided to reduce the risk of barotrauma or gastric insufflation. Under these modified airway conditions, systematic inspection of the pars flaccida was performed. The previously obscured lower fistula became clearly visible and widely patent (figure 3b). An additional proximal fistula was revealed approximately 2 cm above the distal fistula (figure 4).
Positive airway pressure may be particularly helpful when posterior intrusion-type tracheomalacia contributes to intermittent fistula concealment. During spontaneous breathing, dynamic posterior intrusion can narrow the lumen and intermittently obscure a fistulous opening, particularly if the tract has a flap-valve configuration. Conversely, PEEP may splint the posterior membrane away from the opposing tracheal wall, while local low-flow insufflation can transiently distend a collapsed tract and improve direct visualization.
Although posterior tracheal wall manipulation with a rigid bronchoscope may also expose an occult fistulous opening in selected cases, the mechanism differs from the approach demonstrated here. Our approach may better reveal a pressure-dependent fistula while limiting mucosal trauma and mechanical distortion caused by rigid instrumentation.
Alternative adjuncts, such as methylene blue instillation, may assist in fistula localization, but ideally require simultaneous esophageal endoscopy. In this case, low-flow oxygen insufflation provided direct real-time bronchoscopic confirmation of both tracheal openings, obviating the need for further confirmation.
Together, these findings established the diagnosis of type D EA with two TEFs. Definitive surgical repair was then undertaken, and additional intraoperative bronchoscopy subsequently confirmed closure of both fistulas.
Conclusion
This case demonstrates that systematic, physiology-informed bronchoscopy is critical in esophageal atresia, particularly when initial findings appear inconclusive. Dynamic assessment under spontaneous breathing, followed by targeted modification of airway conditions using PEEP and brief intermittent low-flow oxygen insufflation, can unmask otherwise occult proximal fistulas and refine anatomical diagnosis. Such an approach directly impacts surgical planning and may reduce the risk of missed lesions. Incorporating structured preoperative bronchoscopy with deliberate airway manipulation should therefore be considered an essential component of contemporary EA/TEF evaluation.
Conflict of interest
None to declare.
Data availability statement
There is no original data beyond those displayed in the submission.
Author contributions
SLE: Contributed to peri-procedural care, collected clinical data, and wrote the first draft of the manuscript and video narrative.
AA: Performed the surgical procedure, provided peri-operative patient care, coordinated multidisciplinary management, and critically reviewed the manuscript.
MS: Performed the surgical procedure, provided peri-operative patient care, and critically reviewed the manuscript.
ASM: Provided anesthesia management during the procedure, contributed to peri-procedural care, and critically reviewed the manuscript.
PS: Conceived the report, planned the intervention, performed the bronchoscopic procedure, and critically reviewed and edited the manuscript.
All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Ethical statement
The procedure was performed as part of routine clinical care. Institutional policy waived the need for specific ethics committee approval or written informed consent for this case report.
References
1. Conforti A, Valfrè L, Scuglia M, Trozzi M, Meucci D, Sgrò S, Bottero S, Bagolan P. Laryngotracheal abnormalities in esophageal atresia patients: a hidden entity. Front Pediatr. 2018 Dec 18;6:401. doi: 10.3389/fped.2018.00401
2. Parolini F, Boroni G, Stefini S, Agapiti C, Bazzana T, Alberti D. Role of preoperative tracheobronchoscopy in newborns with esophageal atresia: a review. World J Gastrointest Endosc. 2014 Oct 16;6(10):482–7. doi: 10.4253/wjge.v6.i10.482
3. Dingemann C, Eaton S, Aksnes G, Bagolan P, Cross KM, De Coppi P, et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: diagnostics, preoperative, operative, and postoperative management. Eur J Pediatr Surg. 2020 Aug;30(4):326–36. doi: 10.1055/s-0039-1693116
4. Levine H, Schonfeld T, Handelsman S, Bar-On O, Steuer G, Mei-Zahav M, et al. Low flow intermittent bronchoscopic oxygen insufflation to identify occult tracheo-esophageal fistulas. Respir Med. 2021 Sep;186:106544. doi: 10.1016/j.rmed.2021.106544
Submitted: May 14, 2026
Accepted: June 6, 2026
Published: June 24, 2026
© 2026 Less Elazari et al. This open-access article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0).