Design, Development and Assessment of a 3D Printed Pediatric Flexible Bronchoscopy Simulator
Abstract
Pediatric flexible bronchoscopy is a potentially risky procedure that requires realistic training for optimal procedural yield and complication mitigation. Three-dimensional printing represents a promising technology for developing realistic and low-cost surgical training models, but its utility in pediatric flexible bronchoscopy has not been thoroughly explored. A 3D-printed training simulator was developed by computer-aided design including: (1) a synthetic pediatric airway down to the 3rd generation and a distal reservoir to simulate bronchoalveolar lavage and (2) the benchtop enclosure including a mechanical airway and external pegs for simulation of extraluminal airway compression. Using stereolithography, the airway was fabricated with an elastic resin. An external surface finish was applied using silicone-based fabric paint and biocompatible adhesive to match physiologic intraluminal color. The benchtop enclosure was manufactured using polylactic acid via fused deposition modeling. The 3D-printed airway simulator was evaluated alongside a traditional virtual reality bronchoscopy simulator across 6 domains: physical attributes, realism of experience, ability to perform tasks, educational value, relevance to clinical practice, and global assessment. Six fellowship trainees rated the 3D printed airway favorably across all domains and assessments were similar to the traditional virtual reality simulator. The 3D printed airway had a fixed unit material cost of $6.09 for the airway and $17.13 for the benchtop enclosure. This preliminary assessment of a 3D printed pediatric flexible bronchoscopy simulator suggests that it provides a realistic, customizable and cost-effective mechanism for advanced training in pediatric flexible bronchoscopy.
Introduction
Pediatric flexible bronchoscopy (PFB) is an important procedure in pediatric pulmonary and critical care medicine, serving both diagnostic and therapeutic purposes. Procedural competence requires a comprehensive understanding of anatomical structures, instrument manipulation, airway pathology, and management of acute airway complications. While mentored patient clinical experience is essential, providing trainees with sufficient realistic learning opportunities without compromising patient safety presents significant challenges (1,2). Traditional training resources, including cadaveric specimens, animal models, and virtual reality (VR) simulators, have limitations that impede effective and accessible learning experiences (3–6). These limitations include high costs, restricted availability, ethical concerns, and limited anatomical fidelity.
3D printing technology has facilitated the development of procedural simulation models across various medical fields due to its ability to create realistic and customizable models. In interventional cardiology, 3D printed heart models have been valuable for simulating complex procedures and improving procedural planning (7). Similarly, the development of 3D printed facial flap and otoplasty surgical simulators, as well as development of thoughtful curricula around these simulators, have proven beneficial in otolaryngology, enabling trainees to refine their skills in complex surgical techniques (8–10). These achievements underscore the potential for 3D printing technology to improve pediatric bronchoscopy training.
In comparison to traditional VR simulators, the use of 3D printed airways has demonstrated improved affordability, heightened realism, and enhanced haptic feedback (11–13). However, most 3D printed bronchoscopy models are designed for teaching adult rather than pediatric bronchoscopy (14). Pediatric flexible bronchoscopists must be able to identify unique pediatric pathologies such as congenital tracheobronchomalacia and operate with smaller bronchoscopes, cameras, suction ports, and fluid aliquots for bronchoalveolar lavage. By using patient-specific anatomical replicas, 3D printing enables trainees to engage in realistic practice scenarios closely resembling the unique features of the pediatric airway.
This study aimed to develop and assess a low-cost, 3D printed simulation model for pediatric flexible bronchoscopy. Our objective was to compare the performance of a 3D printed airway to a traditional VR model based on evaluations from trainees. We hypothesized that a 3D printed airway specifically designed to simulate pediatric anatomy and pathologies would have similar educational value compared to a traditional VR simulator.
Material and Methods
Simulator Design and Development
The bronchoscopy simulator developed for this study included the synthetic 3D printed airway and the benchtop enclosure. In order to design the anatomically accurate airway model, a de-identified computed tomography (CT) scan of lungs from a 7-year-old child without airways disease was converted into a 3D digital model using the segmentation software Materialise Mimics (Leuven, Belgium). Using computer-aided design (CAD) software, this digital model was modified to include only the relevant airway anatomy from the vocal cords to the third airway generation and further optimized to facilitate 3D printing.
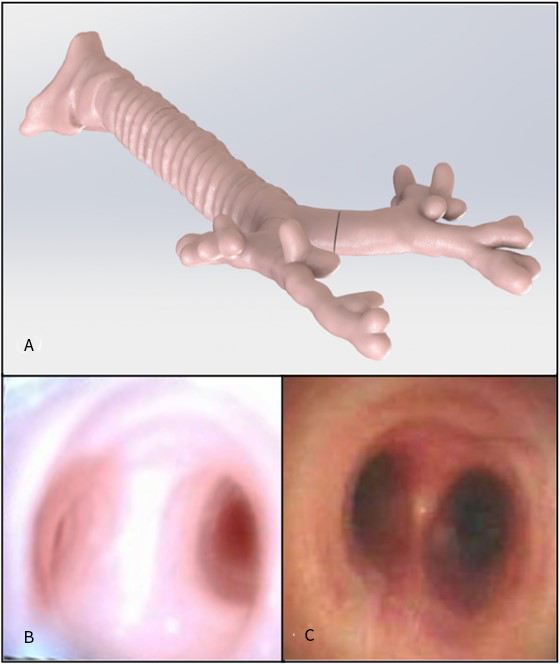
The 3D printed airway was fabricated using stereolithography (SLA) 3D printing, which cures liquid resin into hardened plastic using ultraviolet light. After trialing various materials, the team arrived at an elastic engineering resin with 50A Shore durometer from Formlabs (Somerville, Massachusetts). This material was selected because of the combination of flexibility to accurately simulate the pediatric airway anatomy as well as durability to withstand multiple cycles of use. More rigid materials resulted in increased resistance when navigating to the distal airway and posed an increased risk of bronchoscope damage. A wall thickness of 4 mm resulted in undesirable stiffness and resistance to external compression, while a wall thickness of 1 mm resulted in poor durability during repeated use. Ultimately, a wall thickness of 2 mm offered a suitable balance of compressibility and durability. While the elastic engineering resin achieved the desired mechanical performance, it is only commercially available in a translucent white color which does not offer a realistic intraluminal appearance. An external surface finish was created by blending various silicone-based fabric paints to achieve a desired Pantone PMS 7605 C color that adequately matched the tone of the respiratory mucosa (Figure 1). The airway was further coated with a silicone-based biocompatible adhesive to improve model durability and prevent degradation of the fabric paint.
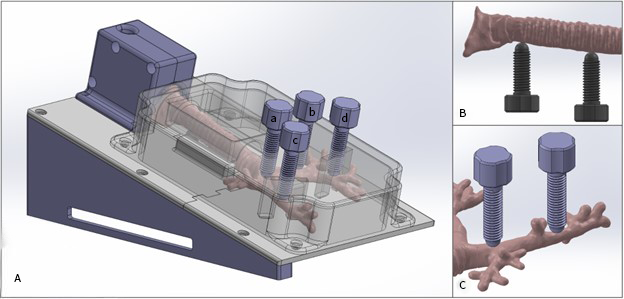
In addition to the airway model, a benchtop enclosure was developed to incorporate additional features into the bronchoscopy simulator and facilitate usability in the training environment. The benchtop enclosure was fabricated using polylactic acid (PLA) via fused deposition modeling (FDM) 3D printing, where a thermoplastic filament is extruded through a heated nozzle and joined together to form a 3D object one layer at a time. First, an opaque housing was designed to conceal the airway so that the operator is unable to view the bronchoscope or reference the anatomy during navigation. Second, a proximal component was integrated into the enclosure with a 7 mm diameter through which a flexible bronchoscope can be inserted. This component was designed to simulate a laryngeal mask airway sitting above the vocal cords. Third, the enclosure was elevated at a 15-degree angle to allow trainees to perform a bronchoalveolar lavage (BAL), in which a 5 mL aliquot of fluid is instilled into the right lower lobe and suctioned for sample collection. The elevation angle was necessary to allow the fluid to flow distally before being recollected. The right lower lobe terminated in a small pouch to accommodate the BAL fluid. Finally, threaded external pegs were incorporated into the body of the enclosure so that compressional force could be applied to the airway at specified anatomical locations to simulate airway compression. Clinical scenarios were designed to teach the diagnosis of tracheomalacia, bronchomalacia, external vascular compression, and other airway pathologies. While the bronchial pegs compress from anterior-to-posterior, the tracheal pegs compress from posterior-to-anterior. This orientation offered the most realistic appearance of bronchomalacia and tracheomalacia (Figure 2).
Simulator Assessment
The simulator was deployed to fellowship trainees in pediatric pulmonology, pediatric surgery, and pediatric critical care medicine. A pediatric pulmonologist (expert bronchoscopist) provided procedural instructions and demonstrated PFB to each of the learners individually using the 3D printed airway and a traditional VR simulator (CAE Incorporated, Montreal, Canada). Participants then performed hands-on training on each model individually with expert just-in-time feedback. While a prior study conducted by our research group investigated the value of integrating the 3D printed airway into a formal fellowship curriculum, this study highlights the development of the 3D printed airway and its educational utility when compared directly to an existing VR simulator (15). The 3D printed airway was designed to teach basic bronchoscopy techniques (e.g., BAL) and simulate pathology (e.g., tracheobronchomalacia). The VR simulator was designed to teach basic bronchoscopy techniques and physiologic airway anatomy. Following their training with both simulators, the fellows completed an assessment adapted from a validated instrument (16) using a 5-point Likert scale across six domains: physical attributes, realism of experience, ability to perform tasks, value, relevance, and global assessment (Table 1). The hypothesis was not shared with the participants. Prior to testing, 9 expert faculty bronchoscopists performed simulated bronchoscopy, evaluated the model using the 6 assessment domains, and agreed that the model was suitable for training.
De-identified data from assessment surveys was collected using Qualtrics software, accessible to participants on their mobile devices immediately after using the bronchoscopy model. Data are described with median and lowest scores of each assessment domain for each of the two simulation models.
Results
Using CAD and 3D printing technology, a realistic, low-cost PFB simulator was developed to teach procedural skills, pulmonary anatomy, common pediatric pathologies (e.g., tracheobronchomalacia), and interventional techniques (e.g., bronchoalveolar lavage).
The model was evaluated by six fellows in pediatric pulmonology, pediatric surgery, and pediatric critical care medicine with nearly no bronchoscopy experience at the beginning of their fellowship training program. The results from the group of fellows are summarized in Table 2.
In general, trainees found the 3D printed airway simulator to be a valuable educational tool across all six domains, suggesting that the model is a promising training model for pediatric pulmonology, critical care, and surgery trainees with limited bronchoscopy experience. Participants assigned scores of 4 and 5 for all domains, suggesting adequacy with room for improvement (Table 2). When comparing the two simulators across all domains, there did not appear to be differences in the median scores.
The 3D printed airway has a fixed unit material cost of $17.13 for the 644 g of PLA material used to fabricate the benchtop enclosure and $6.09 for the 30.6 g of Elastic 50A resin used to construct the airway (Table 3). This estimate does not consider startup expenses for a Form Labs SLA printer with corresponding Elastic 50A resin and a standard FDM 3D printer with corresponding PLA filament. The total print time required for the 3D printed airway is 60 hours 45 minutes. The cost analysis does not include printers, electricity, printer maintenance, post-processing, personnel, or labor.
Discussion
Fellowship trainees in procedural subspecialties without bronchoscopy experience agreed that the 3D printed airway had features that offered educational value that is comparable to a traditional VR simulator. Therefore, a 3D printed airway has potential to offer an educational experience similar to traditional training models at a fraction of the cost and with potential for modifications to reflect unique clinical pathologies.
The 3D printed airway has room for improvement. Participants universally reported a score of “4” or “5” across all domains for both training models. However, whereas 4 out of 6 participants reported that it was “somewhat” easy and 2 out of 6 reported that it was “very easy” to perform tasks with the VR simulator, all participants reported that it was “somewhat” easy to perform tasks with the 3D airway, suggesting some room for improvement with the 3D airway. Durability of the airway will be improved to accommodate more rigorous use that involves repeated external compression from obstruction pegs and saline flushes for bronchoalveolar lavage. Increasing the airway wall thickness from 2 mm to 4 mm resulted in increased airway stiffness and subsequent difficulty with bronchoscope navigation. As such, the team is currently investigating the addition of an external silicone coating to increase durability while preserving model performance. The model was built to teach anatomy of the third generation of airways. With the current design, the 3D printed airway would incur significant resistance with navigation beyond the third generation. Currently, the airway model is fabricated with material that is not compliant when radial forces are applied, unlike the natural airway which is more compliant under these conditions. Additional investigation will need to be conducted to allow the user to navigate to more distal airways, while still preserving the integrity of the model and fidelity of the procedure. External compression pegs offered a simulation of pathologic airway compression. The appearance of the lumen under compression, however, fell somewhat short of the real morphologic appearance of airway malacia or vascular compression. The appearance was limited by the geometry of the external compression peg. Furthermore, dynamic compression of the airways with airflow or cardiac beats was not possible in the static 3D printed airway. Future development will involve designing spring-loaded compression pegs to better simulate a dynamic obstruction and allow the instructor to modify the degree of compression in real time during teaching. Finally, the simulator design could be expanded to incorporate foreign body removal, cryotherapy, or other advanced techniques, which would provide educational value to different specialties such as otolaryngology and thoracic surgery.
Several limitations should be acknowledged in this study. This small study was designed to test the engineering and financial feasibility of this model. It was not designed to offer a robust assessment of its educational value, which would require a larger and more thorough assessment including different testing instruments, learners and experts of variable skill levels and longitudinal skill retention assessments. The instrument itself has limitations: a score of “1”, in some domains, is defined as “Don’t Know”. A Likert scale, however, is designed to express a continuous grade; “Don’t Know” doesn’t adequately fit onto an assessment scale. The instrument was used in its current format since it has been used and validated previously despite its limitations (16). The use of SLA 3D printing for creating the pediatric airway geometry presents a limitation due to the high cost of SLA printers, which contradicts the objective of cost efficiency for the model. Although each individual model costs around $20, the overall implementation costs, including the printers, materials, and labor, might limit implementation at centers without well-established 3D printing labs. Additionally, the study had a small sample size of trainees (n=6). Although efforts were made to align model assessment with previously published works, a small sample size did not lend itself to a robust statistical analysis comparing the two simulation models (17,18).
Conclusion
The development of a low-cost 3D printed pediatric flexible bronchoscopy simulator represents progress in the development of procedural training technology. The simulator offers a realistic, customizable, and cost-effective solution for risk-free surgical skill acquisition in a simulated environment. Ongoing improvements and future directions include integration into a structured curriculum and conducting comprehensive validation studies with diverse participants. To enhance further development of this technology, design files can be made available upon request.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki. This study was exempt from continuing IRB review (HUM00193032).
Conflict of Interest
DA Zopf is a co-founder of MakeMedical, LLC. MakeMedical, LLC has no financial interest in the production of this simulator model. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Data Availability Statement
Design files can be made available upon request to the corresponding author.
Author Contributions
DM, MC, RM, DZ and TS contributed to the development and production of the simulator. TS conducted the learner assessments and oversaw all aspects of the study. All authors were active participants in the writing and editing of the article. All authors read and approved the final manuscript.
Tables
Table 1. 5-point Likert scale survey for the pediatric flexible bronchoscopy simulator evaluation.
| Survey domain | (1) | (2) | (3) | (4) | (5) |
|---|---|---|---|---|---|
| Physical attributes | Don’t know | Not at all realistic | Lacks too many key features | Adequate realism but could be improved | Highly realistic |
| Realism of experience | Don’t know | Not at all realistic | Lacks too many key features | Adequate realism but could be improved | Highly realistic |
| Ability to perform tasks | Too difficult to perform | Very difficult to perform | Difficult to perform | Somewhat easy to perform | Very easy to perform |
| Educational value | Don’t know | No value | Little value | Some value | A great deal of value |
| Relevance to practice | Don’t know | No relevance | Little relevance | Some relevance | Great deal of relevance |
| Global assessment | Poor experience | Requires improvement | Requires small tweaks | Can be used but could be improved | Can be used as is |
Table 2. Median and minimum scores of assessment domains using a 5-point Likert scale (N=6).
| Assessment domain | 3D Airway (median, minimum) | Virtual reality simulator (median, minimum) |
|---|---|---|
| Physical attributes | 5 (5) | 5 (4) |
| Realism of experience | 5 (4) | 5 (5) |
| Ability to perform tasks | 4 (4) | 5 (4) |
| Educational value | 5 (4) | 5 (5) |
| Relevance to clinical practice | 4 (4) | 5 (4) |
| Global assessment | 5 (4) | 5 (4) |
Table 3. Bill of materials for the 3D-printed bronchoscopy model including part cost and print time.
| Part | Qty | Infill | Weight (g) | Material | Cost/g ($) | Part Cost ($) | Print Time (hr) |
|---|---|---|---|---|---|---|---|
| base_1 | 1 | 20% | 72.0 | PLA | 0.03 | 1.80 | 4.97 |
| base_2 | 1 | 20% | 61.0 | PLA | 0.03 | 1.53 | 4.28 |
| base_3 | 1 | 20% | 57.0 | PLA | 0.03 | 1.43 | 4.02 |
| cover | 1 | 20% | 209.0 | PLA | 0.03 | 5.23 | 14.53 |
| decal | 1 | 50% | 12.0 | PLA | 0.03 | 0.30 | 0.88 |
| lma_left | 1 | 20% | 43.0 | PLA | 0.03 | 1.08 | 2.37 |
| lma_right | 1 | 20% | 43.0 | PLA | 0.03 | 1.08 | 2.43 |
| peg_short | 2 | 50% | 8.0 | PLA | 0.03 | 0.40 | 0.48 |
| peg | 4 | 50% | 11.0 | PLA | 0.03 | 1.10 | 0.67 |
| wedge_left | 1 | 20% | 64.0 | PLA | 0.03 | 1.60 | 4.28 |
| wedge_right | 1 | 20% | 64.0 | PLA | 0.03 | 1.60 | 4.28 |
| airway | 1 | 100% | 30.6 | Elastic 50A | 0.20 | 6.09 | 17.57 |
| Total | 23.21 | 60.76 |
References
1. Leong A, Benscoter D, Brewington J, Torres-Silva C, Wood RE. Pediatric flexible airway endoscopy training during a pandemic and beyond: Bending the curve. Pediatr Pulmonol. 2021 Jun;56(6):1386-8. doi: 10.1002/ppul.25311
2. Leong AB, Green CG, Kurland G, Wood RE. A survey of training in pediatric flexible bronchoscopy. Pediatr Pulmonol. 2014 Jun;49(6):605-10. doi: 10.1002/ppul.22872
3. Corbetta L, Arru LB, Mereu C, Pasini V, Patelli M. Competence and training in interventional pulmonology. Panminerva Med. 2019 Sep;61(3):203-31. doi: 10.23736/S0031-0808.18.03562-0
4. Ram B, Oluwole M, Blair RL, Mountain R, Dunkley P, White PS. Surgical simulation: an animal tissue model for training in therapeutic and diagnostic bronchoscopy. J Laryngol Otol. 1999 Feb;113(2):149-51. doi: 10.1017/s0022215100143415
5. Colt HG, Crawford SW, Galbraith O 3rd. Virtual reality bronchoscopy simulation: a revolution in procedural training. Chest. 2001 Oct;120(4):1333-9. doi: 10.1378/chest.120.4.1333
6. Andersen AG, Rahmoui L, Dalsgaard TS, Svendsen MBS, Clementsen PF, Konge L, Bjerrum F. Preparing for Reality: A Randomized Trial on Immersive Virtual Reality for Bronchoscopy Training. Respiration. 2023 Apr;102(4):316-23. doi: 10.1159/000528319
7. Grab M, Hopfner C, Gesenhues A, König F, Haas NA, Hagl C, Curta A, Thierfelder N. Development and Evaluation of 3D-Printed Cardiovascular Phantoms for Interventional Planning and Training. J Vis Exp. 2021 Jan;167:e62063. doi: 10.3791/62063
8. Powell AR, Srinivasan S, Green G, Kim J, Zopf DA. Computer-Aided Design, 3-D-Printed Manufacturing, and Expert Validation of a High-fidelity Facial Flap Surgical Simulator. JAMA Facial Plast Surg. 2019 Jul;21(4):327-31. doi: 10.1001/jamafacial.2019.0050
9. Chang B, Powell A, Ellsperman S, Wehrmann D, Landry A, Jabbour N, Goudy S, Zopf D. Multicenter Advanced Pediatric Otolaryngology Fellowship Prep Surgical Simulation Course with 3D Printed High-Fidelity Models. Otolaryngol Head Neck Surg. 2020 May;162(5):658-65. doi: 10.1177/0194599820913003
10. Michaels RE, Zugris NV, Cin MD, Monovoukas DA, Koka KK, Smith C, Bohm L, Kim J, Green G, Roby B, Jabbour N, Lind M, Goudy S, Zopf DA. A national pediatric otolaryngology fellowship virtual dissection course using 3D printed simulators. Int J Pediatr Otorhinolaryngol. 2022 Aug;162:111273. doi: 10.1016/j.ijporl.2022.111273
11. Ha JF, Morrison RJ, Green GE, Zopf DA. Computer-Aided Design and 3-Dimensional Printing for Costal Cartilage Simulation of Airway Graft Carving. Otolaryngol Head Neck Surg. 2017 Jun;156(6):1044-7. doi: 10.1177/0194599817697048
12. Ho BHK, Chen CJ, Tan GJS, Yeong WY, Tan HKJ, Lim AYH, Ferenczi MA, Mogali SR. Multi-material three dimensional printed models for simulation of bronchoscopy. BMC Med Educ. 2019 Jun;19(1):236. doi: 10.1186/s12909-019-1677-9
13. Pedersen TH, Gysin J, Wegmann A, Osswald M, Ott SR, Theiler L, Greif R. A randomised, controlled trial evaluating a low cost, 3D-printed bronchoscopy simulator. Anaesthesia. 2017 Aug;72(8):1005-9. doi: 10.1111/anae.13951
14. Hornung A, Kumpf M, Baden W, Tsiflikas I, Hofbeck M, Sieverding L. Realistic 3D-Printed Tracheobronchial Tree Model from a 1-Year-Old Girl for Pediatric Bronchoscopy Training. Respiration. 2017 Mar;93(4):293-5. doi: 10.1159/000459631
15. Painter N, Monovoukas D, Delecaris AO, Coverstone AM, Zopf DA, Saba TG. Incorporating a Three-Dimensional Printed Airway into a Pediatric Flexible Bronchoscopy Curriculum. ATS Sch. 2024 Jan;5(1):142-53. doi: 10.34197/ats-scholar.2023-0078OC
16. Barsness KA, Rooney DM, Davis LM. Collaboration in simulation: the development and initial validation of a novel thoracoscopic neonatal simulator. J Pediatr Surg. 2013 Jun;48(6):1232-8. doi: 10.1016/j.jpedsurg.2013.03.015
17. Witsberger CA, Michaels R, Monovoukas D, Cin M, Zugris NV, Nourmohammadi Z, Zopf DA. Development of a High-Fidelity, 3D Printed Otoplasty Surgical Simulator. Ann Otol Rhinol Laryngol. 2023 Jun;132(6):607-13. doi: 10.1177/00034894221105831
18. Artino AR Jr, La Rochelle JS, Dezee KJ, Gehlbach H. Developing questionnaires for educational research: AMEE Guide No. 87. Med Teach. 2014 Jun;36(6):463-74. doi: 10.3109/0142159X.2014.889814