Extracorporeal life support-assisted airway foreign body extraction in an infant: The story of Indian Esperanza, first reported case from India
Abstract
Introduction: Airway foreign body (FB) aspiration in children under the age of three years can be life-threatening. Large airway FB may cause acute airway obstruction requiring immediate intervention. Airway FB extraction carries significant risk to the patient, particularly when the FB are large and or impacted. In cases where the FB cannot be removed, this may result in morbidity and catastrophic events such as cardiac arrest, hypoxic injury or even mortality.
Methods: We report a case of airway obstruction caused by an aspirated chicken bone in an 11-month-old infant. The FB was successfully extracted with the use of extracorporeal membrane oxygenation (ECMO) to maintain oxygenation during the procedure.
Results: Successful removal of the FB was achieved without any significant hypoxia once the patient was placed on ECMO.
Conclusion: Early initiation of ECMO in cases involving large or impacted FB should be considered, especially if there is a perioperative risk of hypoxia due to difficult removal or prolonged procedure. A multidisciplinary team approach clearly has an impact on the outcomes in such cases.
Introduction
Airway foreign bodies (FB) are more common in children between one and five years of age. Large impacted FB in the airways carry a significant risk of mortality in children (1). Airway obstruction can lead to respiratory arrest, which may progress to cardiac arrest due to prolonged hypoxia. Extracorporeal membrane oxygenation (ECMO) is now an established life-assist device for temporarily supporting respiratory or cardiac failure (2, 3). In addition to its multiple indications, its role as a bridge for patient stabilization before FB removal is increasingly being recognized (4-7). We report a case of airway obstruction caused by an aspirated chicken bone in an 11-month-old infant, successfully extracted with the aid of extracorporeal life support (ECLS) to maintain oxygenation during the procedure.
The Institutional Ethics Committee (IEC) was consulted, and the requirement for formal ethical approval was waived.
Case Description
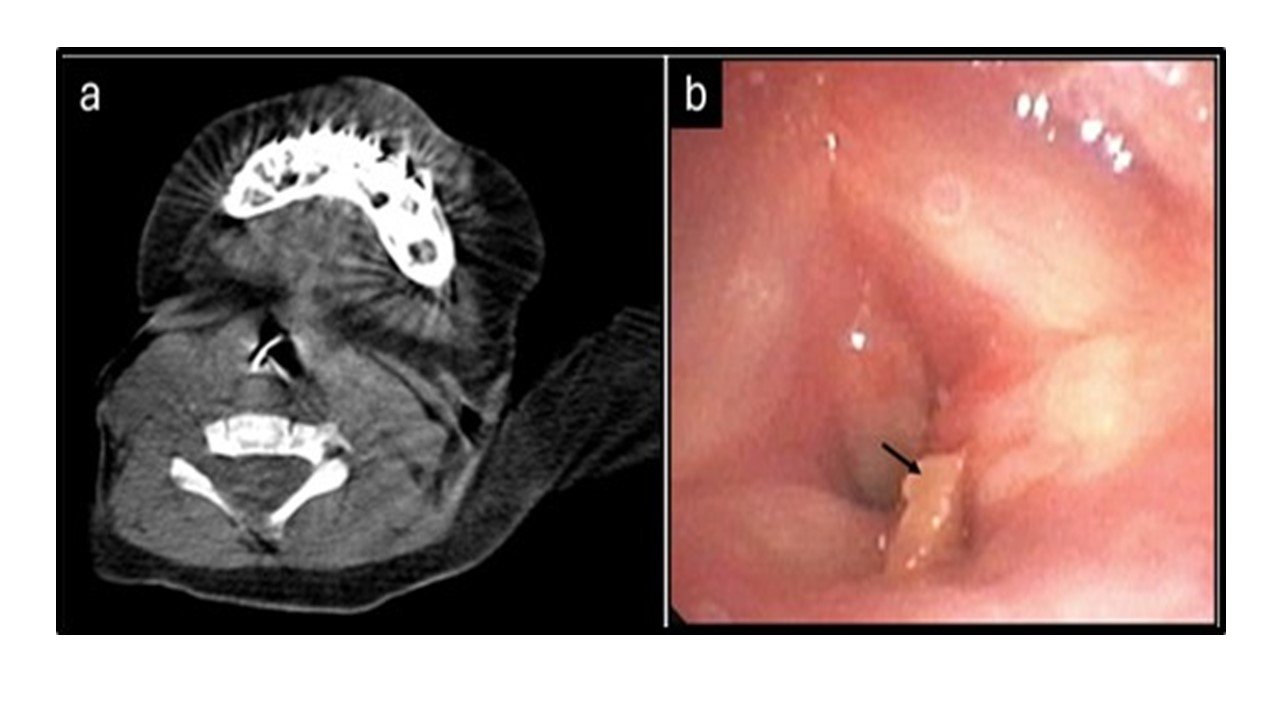
An 11-month-old infant was rushed to the emergency room with complaints of altered sensorium, labored breathing, and audible stridor. The infant had a history of hospital admission at a primary care center over the previous four days with similar complaints, for which she had received supportive care. Detailed history revealed that she had been fed chicken broth a week earlier on a festive occasion. Computed tomography of the chest showed collapse of the left upper lobe and a radio-opaque, irregular opacity suspicious of a FB in the subglottic location (Figure 1A). Diagnostic flexible bronchoscopy using a ultrathin flexible bronchoscope (Olympus BF-XP190, outer diameter 2.8 mm) under conscious sedation confirmed a large obstructing FB immediately below the vocal cords with extension to the vocal cords causing luminal obstruction (Figure 1B).
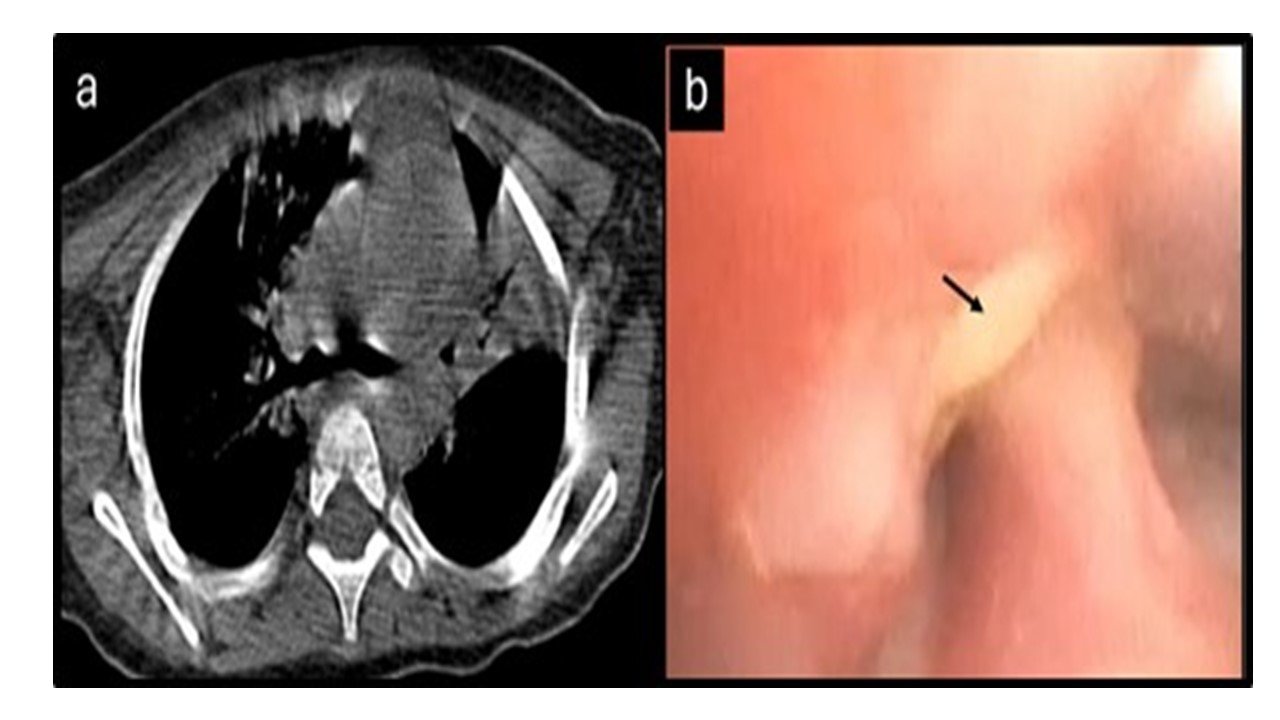
Multiple attempts to extract the FB with rigid and flexible forceps failed as the FB was impacted deep into the mucosa. In view of desaturation, he was intubated using a 3.0 mm uncuffed endotracheal tube to secure the airway. Following intubation, the patient maintained oxygenation for a while; however she developed sudden bradycardia followed by hypoxia leading to asystole, which required one cycle of cardiopulmonary resuscitation (CPR) to achieve return of spontaneous circulation. A repeated chest CT was done to assess the lung condition and FB, which showed displacement of the FB in the right bronchus intermedius with bilateral lower lobe consolidations (Figure 2A). Given the need for CPR due to airway obstruction, extracorporeal membrane oxygenation (ECMO) was initiated, and the infant was placed on veno-arterial extracorporeal life support (VA ECMO) to assist the interventional procedure for removal of the FB from the airways.
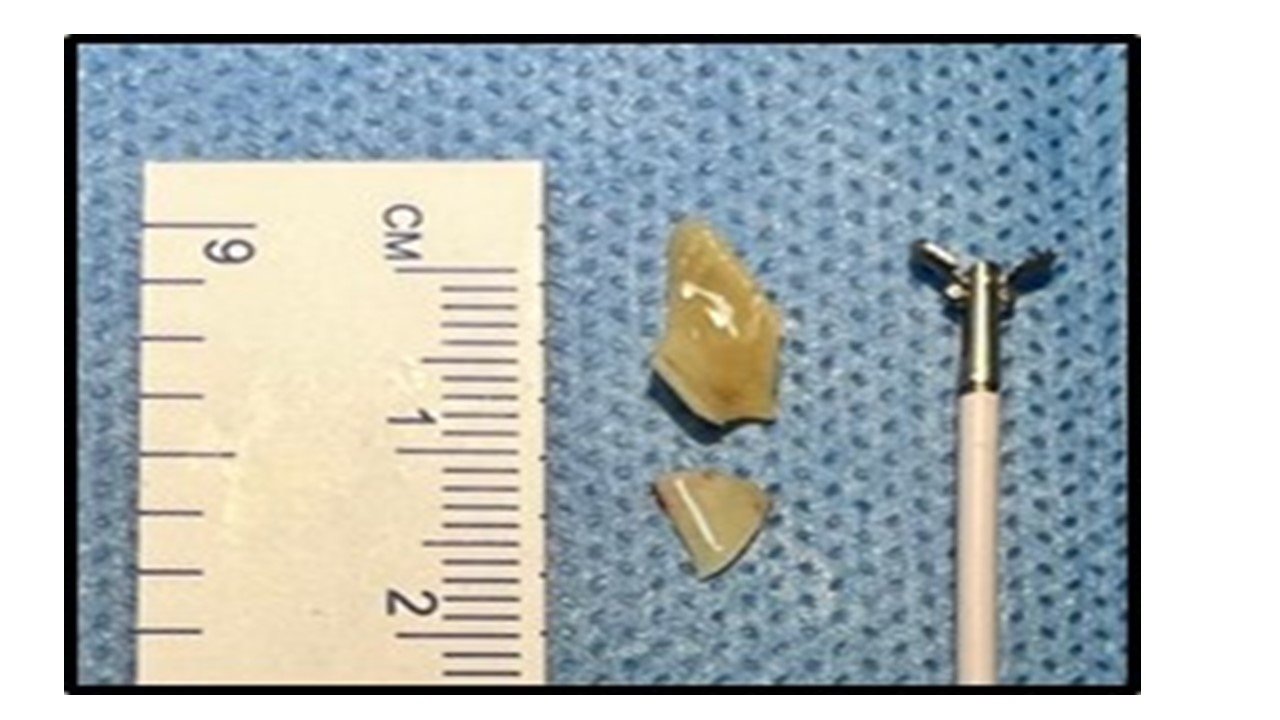
She was initiated on VA ECMO with right internal jugular vein (12 Fr cannula, Edwards Lifesciences) and right common carotid (10 Fr cannula, Medtronic Bio-Medicus) by surgical cutdown, with flows at 0.4L/min and sweep gas of 1 L/min (Maquet Getinge group). Upon ECMO initiation, oxygenation was maintained, and the endotracheal tube was removed. Bronchoscopy was performed using an ultrathin bronchoscope (Olympus BF-MP190F, outer diameter 3.0 mm), which showed pooled secretions in the tracheobronchial tree. A FB was found at the right bronchus intermedius extending to the opening of the right lower lobe bronchi (Figure 2B). Using a flexible bronchoscope (Olympus BF-P190, outer diameter 4.2 mm), the FB (chicken bone) was successfully extracted in two pieces, restoring luminal patency (Figure 3) via a laryngeal mask airway (LMA) as the airway conduit.
The patient was then electively intubated using a 3.5 mm uncuffed endotracheal tube (ET) in view of significant edema in the subglottic space following intervention. With the initiation of mechanical ventilation, ECMO was gradually weaned, and the patient was decannulated in the operating theatre. She was subsequently weaned from mechanical ventilation support the following day and was discharged on the 4th day following admission with a room air oxygen saturation of 96% in a stable condition. The parents were counselled on optimal feeding practices.
Discussion
ECMO is a life-assist device used for temporarily supporting respiratory or cardiac failure. The use of ECMO began in 1954 in cardiac surgery and its first application for respiratory failure was reported in 1972 (2). Since then, multiple uses of ECMO for respiratory failure have been developed, the most common being acute respiratory distress syndrome (ARDS), pneumonia, and sepsis. During the COVID-19 pandemic, ECMO was widely used as a supportive measure for respiratory failure. (2, 3).
There are two main types of ECMO: veno-arterial (VA-ECMO), used for cardiac failure and veno-venous (VV-ECMO), used for respiratory failure (3). According to the Extracorporeal Life Support Organization (ELSO) guidelines, the use of ECMO is recommended for patients with respiratory failure under specific indications (4). With the growing indications of ECMO, its use has been extended to pediatric and neonatal patients as well (5). The use of ECMO in this age group began with pediatric cardiac surgery cases and later expanded as a bridge to cardiac transplants in cardiomyopathy patients (6). ECMO is now used for various pediatric indications, the most common being pneumonia, aspiration, or sepsis. Neonatal indications have included neonatal respiratory distress syndrome, persistent pulmonary hypertension of the newborns, congenital diaphragmatic hernia, and meconium aspiration syndrome (7).
Another vital indication for ECMO is its use in CPR, referred to as extracorporeal cardiopulmonary resuscitation (ECPR), where it rescues patients with sudden cardiac arrest intractable to the standard life support protocol (7, 8). Shakoor et al., in a single-centre retrospective study on the use of ECPR in the pediatric population, included 70 patients who documented a 70% survival to decannulation and a 54% to discharge (9). Our patient was an 11-month-old infant who experienced cardiac arrest following hypoxia due to a FB in the airway. As a bridge to FB removal, ECPR was conducted and the patient was successfully oxygenated until the FB was removed. There have been only a handful of documented instances where ECMO was utilized for stabilizing patients prior to FB removal. Such cases are particularly rare in infants. Most cases reported in the literature presented to the emergency department with respiratory distress. Many of these patients either suffered cardiac arrest during admission or were unresponsive on presentation (10,11).
The procedure of ECMO involves extensive monitoring due to anticoagulation required by the system itself, and the hemodynamics of paediatric patients are usually complex. This places the infant at increased risk for life-threatening coagulopathy complications like bleeding and thrombosis. Hence, appropriate expertise is required for managing a paediatric patient on ECMO. This case represents a rare occurrence globally and stands as a pioneering indication of ECMO utilization as a temporary life support measure within our country's medical landscape. The patient was decannulated in the theatre and discharged home on day four with no hypoxic or residual damage. This case report highlights that one should not avoid using ECMO beyond its standard indications, as it is the most crucial life-saving tool currently available.
Airway FB aspiration carries a potential life risk during extraction, especially when the objects are too large or impacted for a prolonged period of time. ECLS stabilizes oxygenation, thereby giveing time to the operator to make appropriate decisions for extraction, as in this case. This case recalls the first neonatal patient, Esperanza, who received successful ECMO treatment for ARDS in 1975 (12).
Conclusion
Extracorporeal life support should be considered a stabilization measure when airway intervention procedures carry significant perioperative risks. It is important that early decisions regarding ECMO are made in cases of critical airway obstruction with involvement of a multidisciplinary team.
Conflict of interest
The authors have no conflict of interest to disclose.
Data availability statement
This is a case report with no additional data besides that mentioned in the manuscript. However, if needed the authors ill be happy to respond to any suitable query related to data.
Author contributions
HG: Resources, conceptualization, data curation, investigation, formal analysis, writing original draft, visualization;
BPV, VV, SG, TVN, NRNR, RP, S: Resources, review & editing;
SA: Data curation, investigation, formal analysis, review & editing.
All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
References
1. Karišik M. Foreign body aspiration and ingestion in children. Acta Clin Croat. 2023 Apr;62(Suppl1):105-12. doi: 10.20471/acc.2023.62.s1.13
2. Chaves RC, Rabello Filho R, Timenetsky KT, Moreira FT, Vilanova LC, Bravim BD, Serpa A, Corrêa TD. Extracorporeal membrane oxygenation: a literature review. Rev Bras Ter Intensiva. 2019 Oct;31(3):410-24. doi: 10.5935/0103-507X.20190063
3. Wrisinger WC, Thompson SL. Basics of Extracorporeal Membrane Oxygenation. Surg Clin North Am. 2022 Feb;102(1):23-35. doi: 10.1016/j.suc.2021.09.001
4. Tonna JE, Abrams D, Brodie D, Greenwood JC, Mateo-Sidron JA, Usman A, Fan E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO Journal. 2021 Jun;67(6):601-10. doi: 10.1097/MAT.0000000000001432
5. Erdil T, Lemme F, Konetzka A, Cavigelli-Brunner A, Niesse O, Dave H, Hasenclever P, Hübler M, Schweiger M. Extracorporeal membrane oxygenation support in pediatrics. Ann Cardiothorac Surg. 2019 Jan;8(1):109-15. doi: 10.21037/acs.2018.09.08
6. Roeleveld PP, Mendonca M. Neonatal Cardiac ECMO in 2019 and Beyond. Front Pediatr. 2019 Aug 21;7:327. doi: 10.3389/fped.2019.00327
7. Mahmood B, Newton D, Pallotto EK. Current trends in neonatal ECMO. Semin Perinatol. 2018 Mar;42(2):80-8. doi: 10.1053/j.semperi.2017.12.003
8. Prodhan P, Fiser RT, Dyamenahalli U, Gossett J, Imamura M, Jaquiss RD, Bhutta AT. Outcomes after extracorporeal cardiopulmonary resuscitation (ECPR) following refractory pediatric cardiac arrest in the intensive care unit. Resuscitation. 2009 Oct;80(10):1124-9. doi: 10.1016/j.resuscitation.2009.07.004
9. Shakoor A, Pedroso FE, Jacobs SE, Okochi S, Zenilman A, Cheung EW, Middlesworth W. Extracorporeal Cardiopulmonary Resuscitation (ECPR) in Infants and Children: A Single-Center Retrospective Study. World J Pediatr Congenit Heart Surg. 2019 Sep;10(5):582-9. doi: 10.1177/2150135119862598
10. Anton-Martin P, Bhattarai P, Rycus P, Raman L, Potera R. The Use of Extracorporeal Membrane Oxygenation in Life-Threatening Foreign Body Aspiration: Case Series, Review of Extracorporeal Life Support Organization Registry Data, and Systematic Literature Review. J Emerg Med. 2019 May;56(5):523-9. doi: 10.1016/j.jemermed.2019.01.036
11. Park AH, Tunkel DE, Park E, Barnhart D, Liu E, Lee J, Black R. Management of complicated airway foreign body aspiration using extracorporeal membrane oxygenation (ECMO). Int J Pediatr Otorhinolaryngol. 2014 Dec;78(12):2319-21. doi: 10.1016/j.ijporl.2014.10.021
12. Bartlett RH. Esperanza: The First Neonatal ECMO Patient. ASAIO Journal. 2017 Nov-Dec;63(6):832-43. doi: 10.1097/MAT.0000000000000697
Submitted: January 24, 2025
Accepted: August 31, 2025
Published: September 10, 2025
© 2025 Kishan Gonuguntla et al. This open-access article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0).